We would like to use a real-world example of a radiology network struggling to scale, where imaging volume keeps growing but hiring more radiologists simply isn't a viable solution. This is the problem NeuraScan AI is built to solve.
1. The Problem
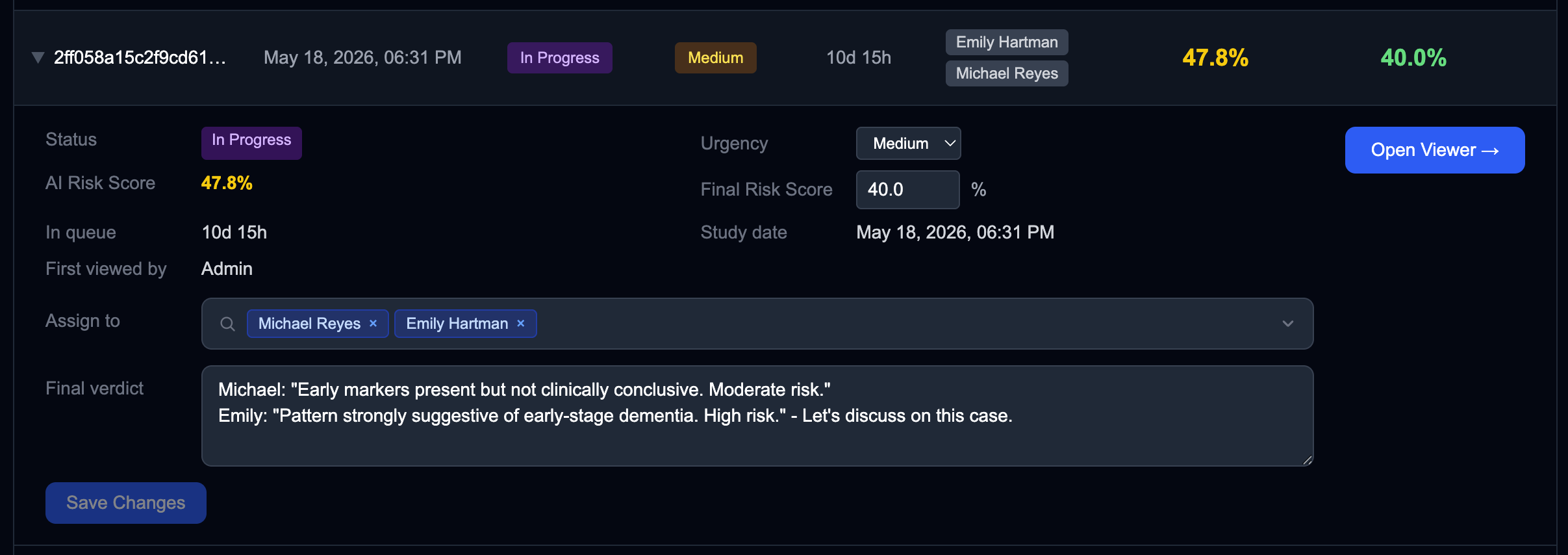
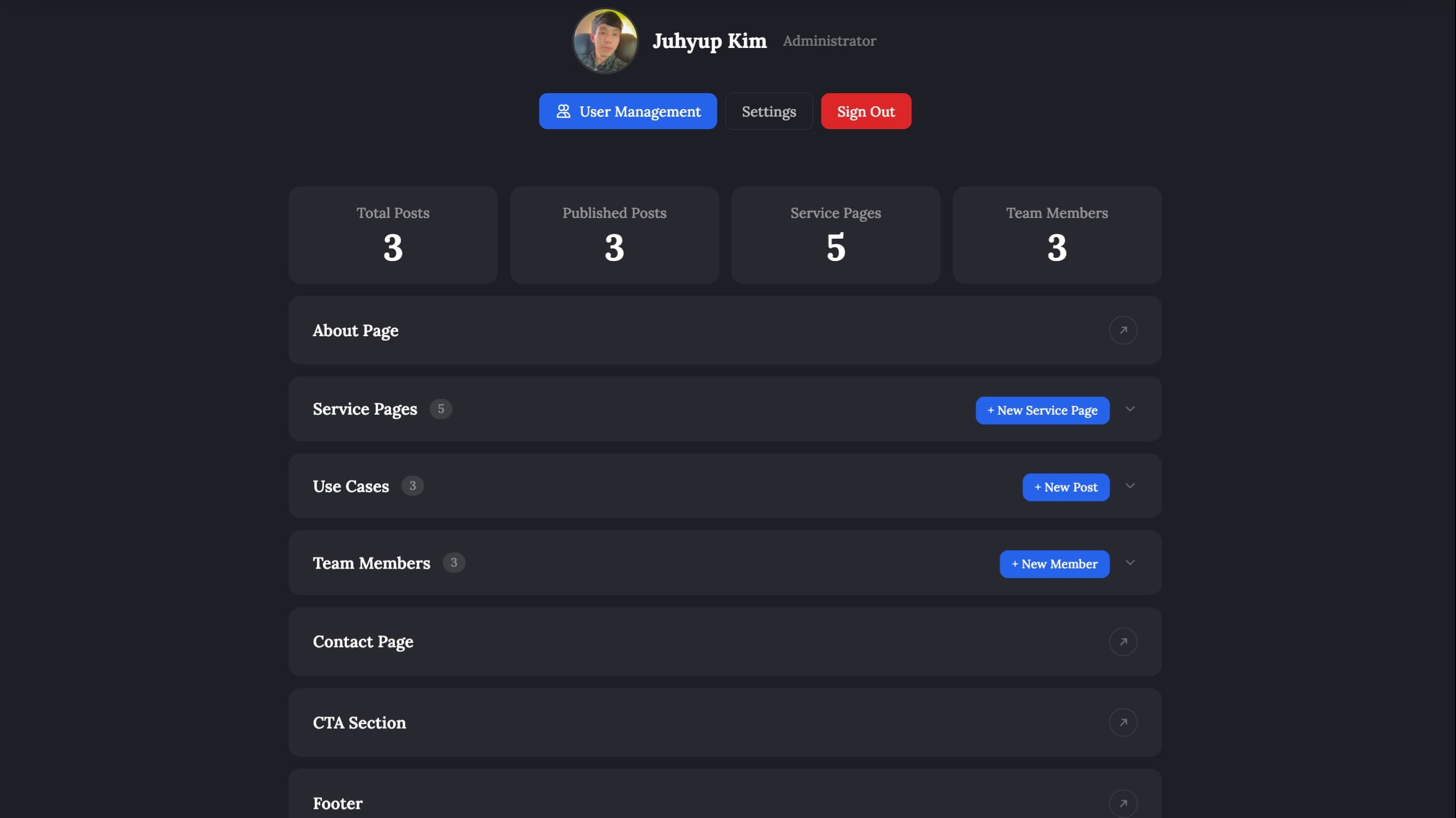
Figure 1: An AI & Human Diagnostics Example
For a radiology network facing rising case volumes, scaling by hiring more radiologists is not a viable strategy. They are specialized clinicians. Their time belongs in diagnosis, not operations.
1.1. Operational
Case queues are unstructured, with no prioritization or urgency signal.
Status tracking across hundreds of active cases is done manually.
Handoffs between radiologist, manager, and referring hospital are inconsistent and error prone.
1.2. Search and Retrieval
Freeform text descriptions make searching prior cases nearly impossible at scale.
Querying by clinical intent is extremely difficult; exact keywords are the only option.
1.3. Scalability
Throughput is entirely headcount dependent. Volume up means staff up.
Triaging or pre-screening cases before a radiologist touches them is extremely difficult without dedicated tooling.
New radiologists onboard into the same broken workflow with no structural improvement.
1.4. Clinical Confidence
AI outputs rarely explain how a score was derived, making them hard to trust.
Validating or challenging an AI recommendation is extremely difficult without a proper audit trail.
Inconsistent diagnostic language across clinicians makes reliable case comparison nearly impossible.
2. What We Built
NeuraScan AI is a medical imaging platform that increases diagnostic throughput, reduces operational overhead, and gives radiologists more time for the clinical work that actually requires their expertise.
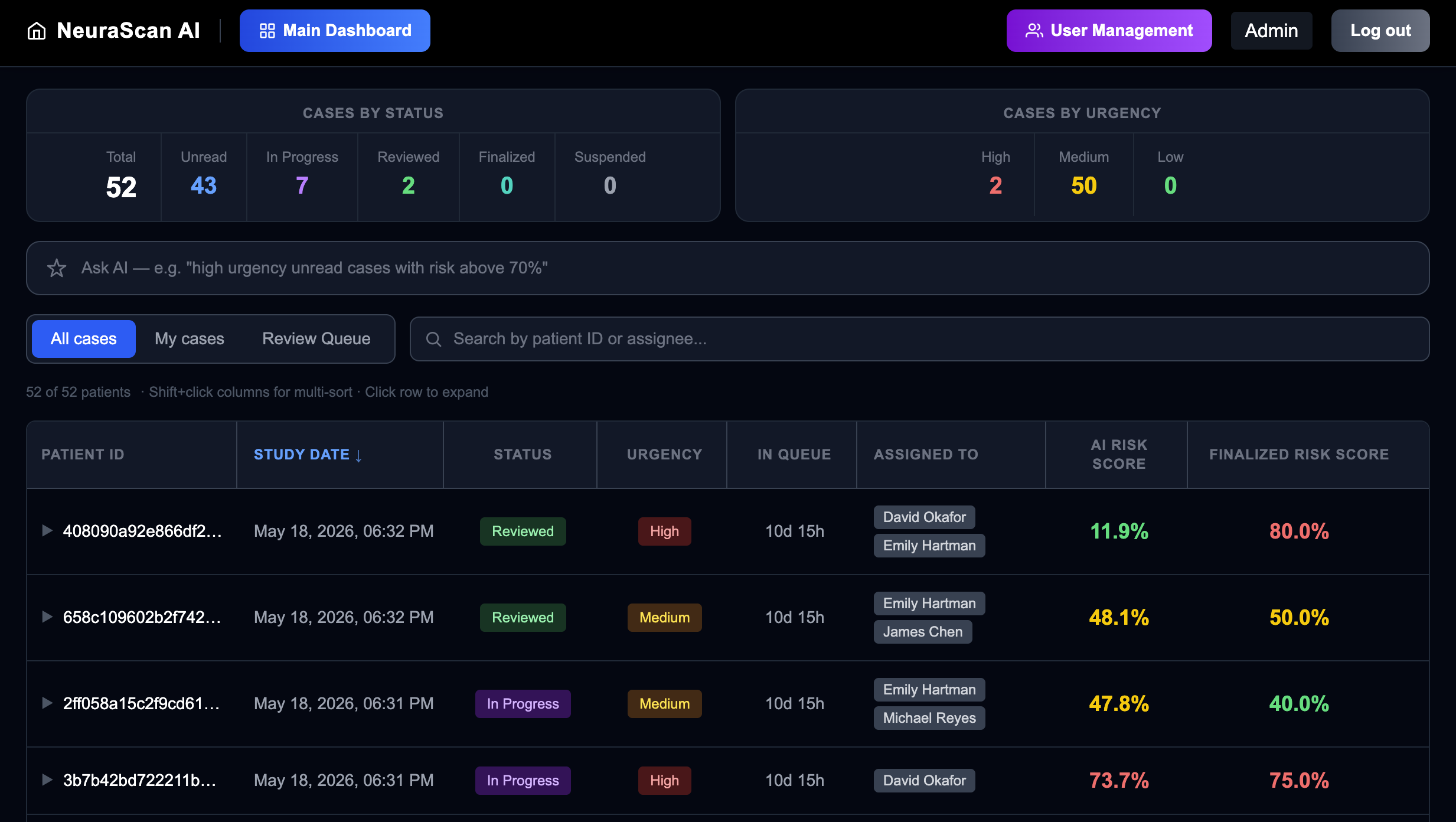
Figure 2: NeuraScan AI Main Dashboard
We restructured the diagnostic process from the ground up:
A computer vision AI engine analyzes every case first, producing a risk score through a comprehensive ensemble voting mechanism before any radiologist is involved.
Each case can be assigned to multiple clinicians, enabling collaborative review and reducing single-point diagnostic risk.
Managers can run intelligent natural language searches across the entire case archive, including complex conditions such as conflicting diagnoses between clinicians or between a clinician and the AI, surfacing the cases that need the closest human attention.
The entire platform is built to institutional security standards, with encrypted Protected Health Information (PHI) handling, immutable audit logs, and strict role-based access control throughout.
2.1. AI Engine
Analyzes every MRI slice and uses a voting mechanism across all slices to produce a final probability score, giving radiologists a data-driven baseline before they begin their review.
Voting across multiple slices reduces the impact of scan noise and positional variation on the final result.
The score is ready before the radiologist opens the case.
2.2. Case Workflow
Every case moves through a structured lifecycle: Unread, In Progress, Reviewed, Finalized, Suspended.
The dashboard gives a real-time view of every case with assigned clinician, urgency, status, study date, encrypted patient ID, and AI Risk Score.
Fully filterable and searchable across all fields in combination.
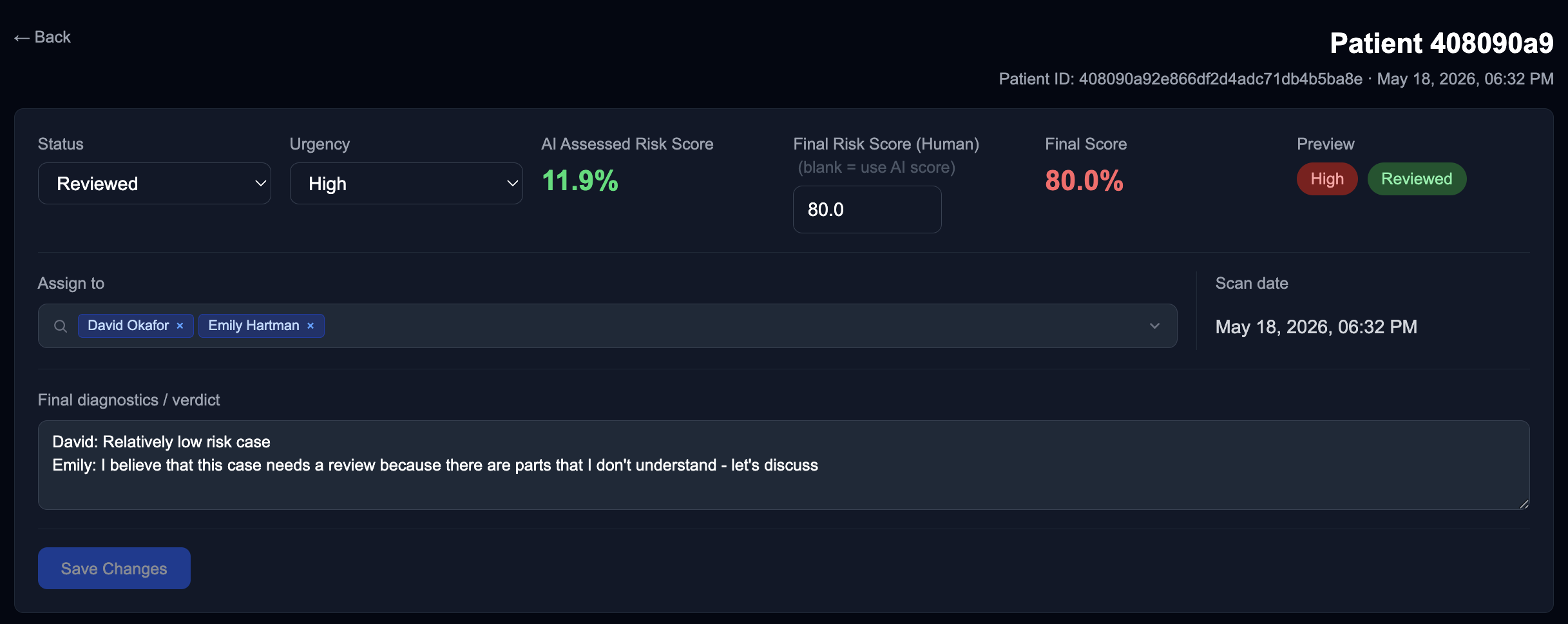
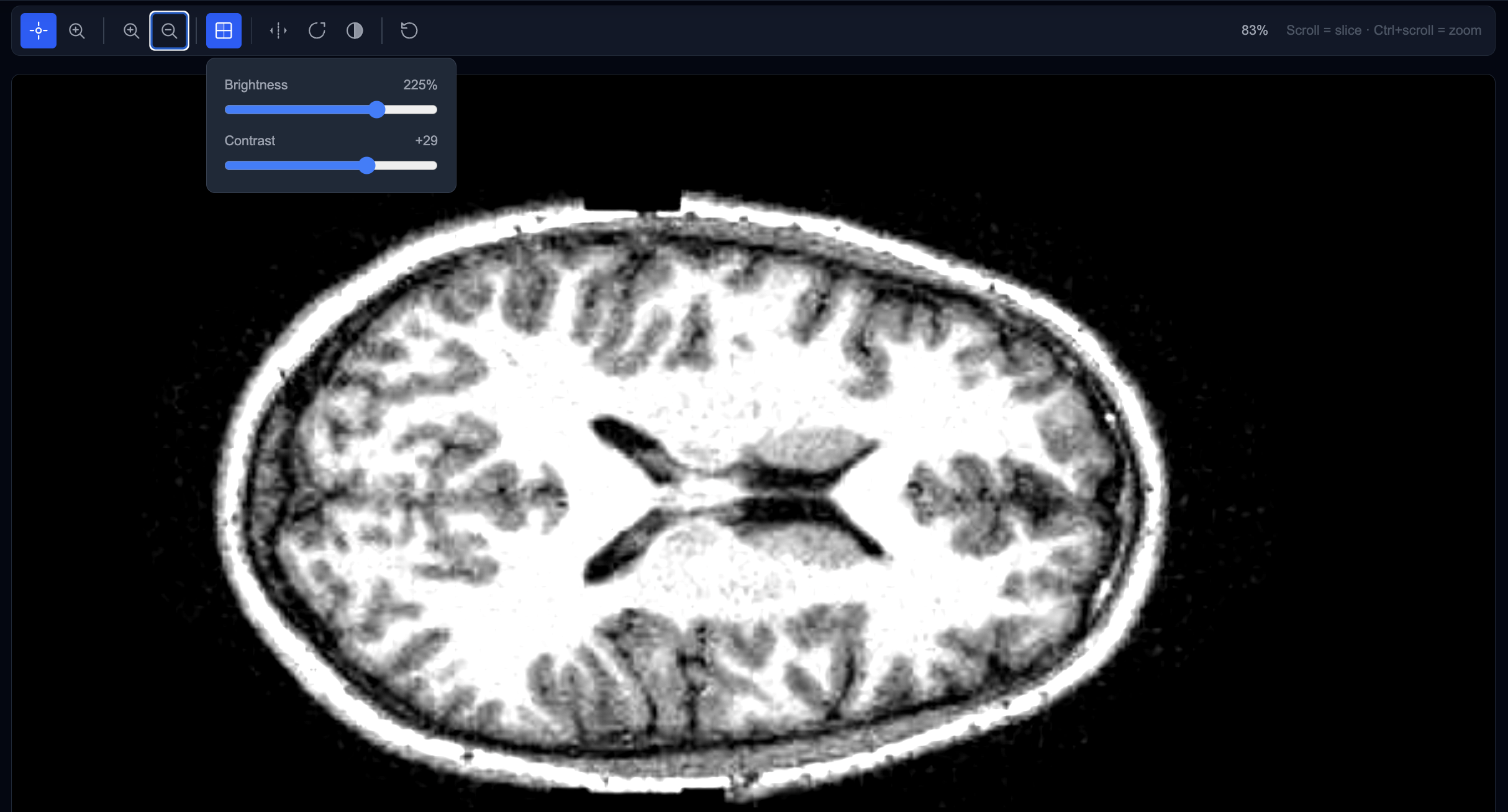
Figure 3: NeuraScan AI Detailed View used for Diagnostics
2.3. LLM Search
Radiologists search in plain language, describing clinical conditions exactly as they would to a colleague.
The LLM matches intent across all case records regardless of how the original descriptions were worded.
Makes large case archives searchable at scale.
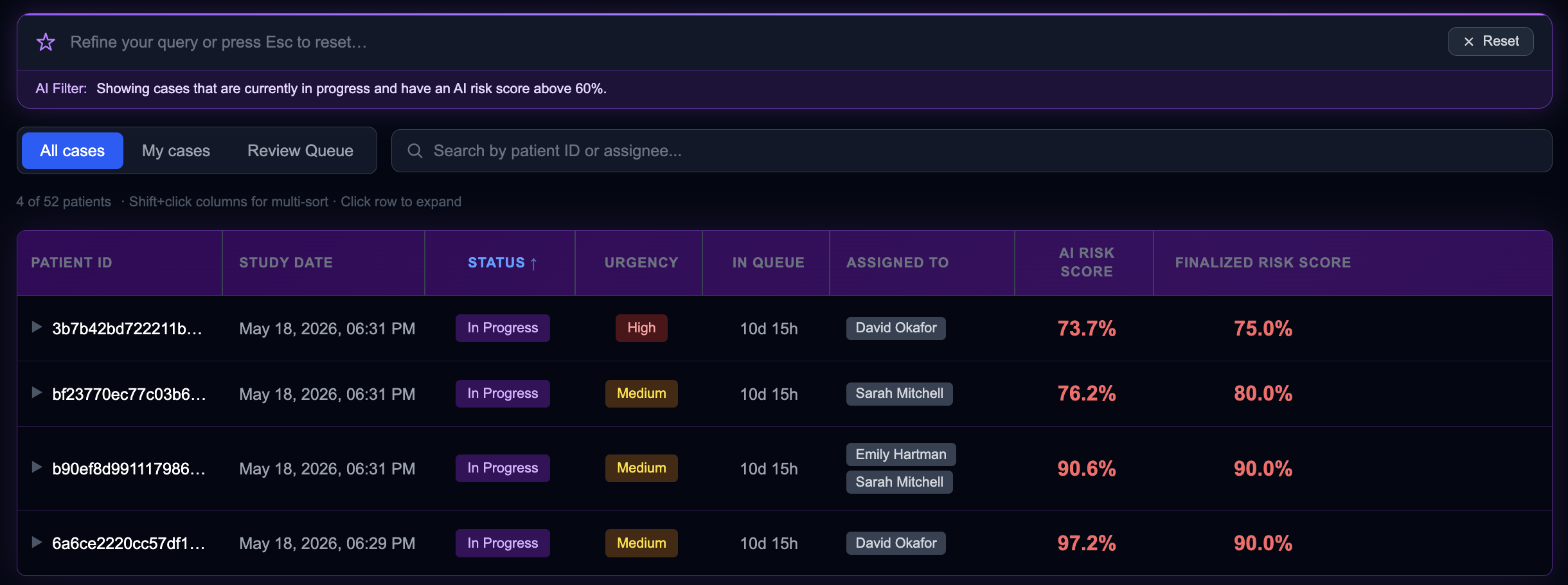
Figure 4: Example of LLM-Search Results
2.4. Access Control: Three-Tier Model
Radiologist: assigned cases only.
Manager: reviews and authorizes finalized reports.
Administrator: account management, permissions, and decrypted audit logs.
Access is strictly scoped to each role. No role can escalate its own permissions.
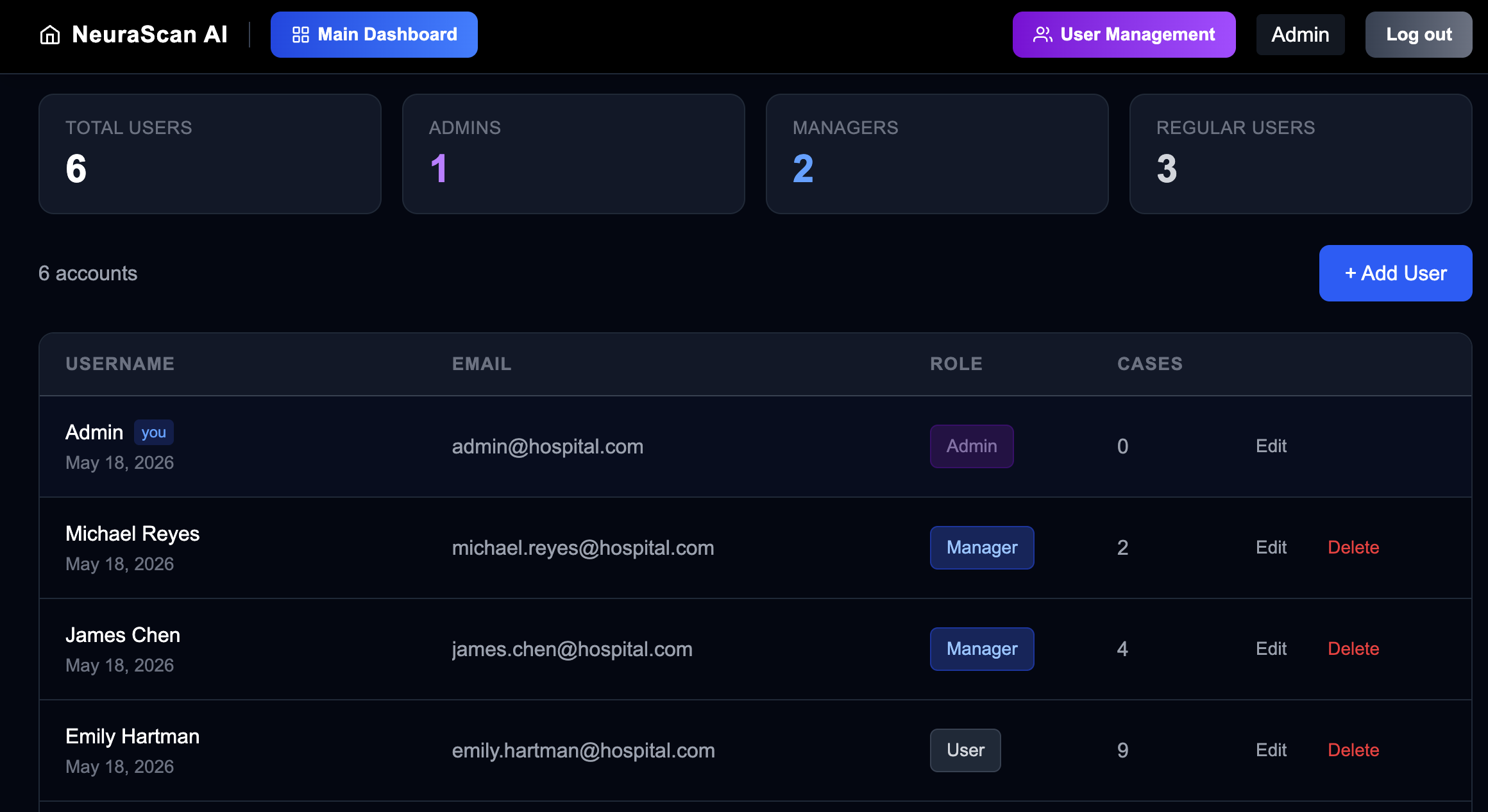
Figure 5: Role-Based Access Control (RBAC) Admin Page
2.5. Report Flow
Radiologist enters a finalized risk score and clinical verdict.
Manager reviews and authorizes before anything leaves the platform.
Output is transmitted back to the referring hospital.
Every step is logged and traceable end to end.
3. Data Engineering
3.1. Ingestion
Compatible with a variety of hospital imaging APIs and data sources.
MRI scans and patient records are pulled automatically the moment a study is ready.
No manual upload, no batch delay.
3.2. Protected Health Information (PHI) Handling
Patient identifying information is encrypted at the point of ingestion.
Users never interact with raw PHI, not in the UI, not in logs.
Encryption at rest (AES-256) and in transit (TLS 1.3).
Architected to meet HIPAA compliance standards.
3.3. Audit and Traceability
Every action is timestamped and audit-logged.
Immutable log chain with full traceability across every step.
Decrypted audit access is restricted to the Administrator role only.
4. The Result
Radiologists spend less time on triage, sorting, and coordination, and more time on diagnosis.
The AI Risk Score sharpens clinical judgment. It does not replace it.
LLM search makes large case volumes manageable without adding headcount.
Full audit trail and role-based access control built for institutional and regulatory environments.
NeuraScan AI is one example of what we build. We work closely with clients in a variety of domains to deliver AI solutions that solve real operational problems.
Bring us your domain, your data, and your constraints, and we will engineer the solution together.